Wine consumption in the context of a healthy lifestyle and cancer risk
Summary
We do not drink only wine/alcoholic beverages, we eat other foods and have particular lifestyle habits. Considering wine/alcohol consumption in the context of the Mediterranean diet and a healthy lifestyle, no increased risk with light to moderate consumption is observed. When reviewing the scientific evidence of the cancer risk with the moderate consumption of alcoholic beverages in isolation, there seems to be a small increase in the risk of breast and colorectal cancer.
There are not enough data to proclaim/support an increased risk of cancer when wine is moderately consumed during the meals and as part of a Mediterranean diet and healthy lifestyle. Such a drinking and dietary pattern seems to result in more health and societal benefits than harm. Moreover, this appears even more pronounced when focusing not only on the life expectancy but also on the increased years without any major diseases such as cardiovascular diseases, diabetes, and cancer with this kind of diet and lifestyle.
When assessing the cancer risk of wine consumption or indeed any other food, it is important to consider it within the context of the cultural, drinking, and dietary habits. Only then, objective conclusions can be drawn.
Furthermore, a lower total mortality among light to moderate drinkers in comparison to lifetime abstainers is found and cannot be ignored. Not only cancer risk, but also risk of other major diseases causing disability and death needs to be taken into consideration. Coronary heart disease, ischemic stroke, diabetes, and dementia, for example, occur less frequently among moderate drinkers than among non-drinkers.
1. Are alcoholic beverages and wine a risk factor for cancers? An ambivalent topic
Cancers are a multifactorial disease and it is increasingly accepted that certain lifestyle choices can affect the risk of developing a cancer. Besides several unmodifiable risk factors (such as age, sex, ethnicity and genetic disposition) which may contribute to an increased risk for the majority of cancers, improvement of lifestyle habits may contribute to a reduced risk of cancer.
According to World Health Organisation (WHO) and the World Cancer Research Fund (WCRF 2018), one third of the cancers could be prevented by adopting a healthy lifestyle (such as avoiding smoking, maintaining a normal body weight, being physically active, avoiding excessive consumption of alcoholic beverages and keeping a healthy dietary pattern) (WHO 2017, WCRF 2018).
In addition, a study performed by the Harvard University further suggested that moderate consumption of alcoholic beverages is one of the five healthy lifestyle factors that reduce the risk of death from all causes, including cancer (Li et al 2018), where the number of low-risk behaviours adopted was inversely related to the risk for mortality.
Furthermore, the Mediterranean Diet (Med Diet) is considered as one of the healthiest in the world by the WHO, that notes that it is directly associated with a lower rate of mortality thanks to its effects on disease prevention (WHO Europe 2018). However, moderate consumption of alcoholic beverages, particularly wine, is an important component of that diet.
So, recommendations for a “healthy” lifestyle which include a healthy diet and avoidance of alcohol, may be confusing, at least from the Med Diet perspective.
Both, the International Agency for Research on Cancer (IARC) and the World Cancer Research Foundation (WCRF) report that alcohol consumption is associated with an increased risk for certain cancers (WCRF 2018, IARC 2012). Risk is elevated with heavier drinking for all alcohol-associated cancers, with the exception of breast cancer that merits a special consideration (see later). In this context, we should remember that the risk of developing cancer involves various risk factors and all cancers that have been associated with alcohol also occur in the absence of drinking.
Some population studies suggested that ANY consumption of an alcoholic beverage was harmful to health, because of increased cancer risk, regardless of the amount consumed and without assessing the pattern of consumption, the type of alcoholic beverage and other lifestyle factors (Gakidou et GBD collaborators 2018, Wood et al 2018).
These authors concluded that it would be best for our overall health to avoid drinking at all, despite the fact that a reduced risk of myocardial infarction and of all-cause mortality was found, and that cardiovascular diseases are the number one cause of death globally (WHO 2017).
Can we still enjoy a glass of wine with the meal without jeopardizing our health? What does the scientific evidence say regarding a possible cancer risk when wine is consumed moderately within the context (“umbrella”) of a healthy lifestyle and a Mediterranean-style diet?
What do we know – Science evidence
The chemical substance ethanol/alcohol
The chemical substance ethanol, also referred to as ethyl-alcohol or alcohol per se has been classified as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC 1988). This classification is given to agents or exposures where the agency considers there to be sufficient evidence of its carcinogenic effects in humans (IARC 1988).
Alcohol metabolism
Two enzymes primarily in the liver, alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH), are involved in breaking down alcohol to enable it to be eliminated it from the body. In the first step, ADH metabolises alcohol into acetaldehyde, which is a highly toxic chemical substance and known carcinogen. Then in a second step, acetaldehyde is further metabolised by ALDH to another, less active metabolite called acetate, which is then further broken down into water and carbon dioxide for elimination from the body. The damage that acetaldehyde can cause to the cells in the body depends on how quickly it is broken down in the first step into acetate (Stockley et al 2010).

Alcohol is absorbed into the blood from the gastrointestinal tract by passive diffusion. On consumption, a small amount of alcohol is absorbed in the mouth and stomach, but most of the absorption takes place in the small intestine. Usually, 30–45 minutes after consumption, the absorption of alcohol is at its maximum. The blood alcohol concentration (BAC) reached depends on several factors:
- the amount consumed,
- the rate at which the amount is consumed,
- gender,
- body mass,
- ethnicity
- recent food intake and
- type of alcoholic beverage consumed.
The BAC reaches higher levels when both larger volumes of alcoholic beverages or higher alcohol percentage (ABV) are consumed. Alcohol distributes from the blood into all tissues and fluids throughout the body in proportion to their relative content of water.
When drinking the same quantity of alcohol, women usually reach a higher BAC level than men, mostly because of their overall lower percentage of body water and higher percentage of body fat, and average lower body weight compared to men. Similarly, lean body mass and total body water is reduced in elderly individuals compared to younger individuals, leading to a relatively higher BAC.
Another important factor in predicting a person’s BAC level is recent food intake. The same amount of alcohol can produce a BAC as much as 50% lower in a person who has recently eaten compared with a person who is drinking on an empty stomach. The balance between the absorption and breakdown of alcohol determines how the BAC changes over time. Most of the alcohol is metabolised for elimination by the liver. As described earlier, alcohol elimination is typically driven by specific alcohol-metabolising enzymes: alcohol dehydrogenase (ADH) and acetaldehyde dehydrogenase (ALDH). This enzyme system, however, becomes saturated at relatively low concentrations of alcohol.
Therefore, during periods of heavy and binge drinking, the liver’s microsomal ethanol oxidizing system (MEOS), an alternative pathway of alcohol metabolism, gets involved and breaks down the excess ingested ethanol to help clear the ethanol faster from the body. During this process, however, free radicals (very reactive oxygen molecules) are created which can damage the cells of the liver (Cederbaum 2012).
What is cancer?
Cancer is a term used for a certain group of diseases in which abnormal cells divide without control and are able to invade other body tissues and organs. Tumours form when unimpeded abnormal cell growth occurs over a period of time. Cancer cells can subsequently spread to other parts of the body through the blood and lymph systems forming secondary malignant tumours or metastases.
There are more than 100 different types of cancers and most cancers are named after the organ or type of cell in which they start.
Benign tumours do not spread, and eventually stop growing.
(https://www.cancer.gov/about-cancer/understanding/what-is-cancer)
Mechanism of alcohol in the cancer development
Researchers have hypothesized multiple ways that alcohol may increase the risk of certain cancers:
- When alcohol is consumed, it is broken down into a toxic chemical substance called acetaldehyde. Acetaldehyde can damage DNA (the genetic material that makes up genes) inside our cells and can further avoid the repair of this damage in the DNA. This is important because it allows cancer to develop.
- Generation of free radicals (chemically reactive molecules that may contain oxygen), which can additionally damage DNA, proteins, and lipids (fats) in the body through a process called oxidation, when oxygen containing radicals are involved, which is exacerbated by the presence of alcohol and acetaldehyde, particularly at higher BAC levels (above approx. 0.5-0.8 ‰, Gessner et al 2019, Ströhle et al 2012).
- Alcohol can impair the body’s ability to break down and absorb a variety of nutrients that may be associated with cancer risk, including vitamin A; nutrients in the vitamin B complex, such as folate, niacin and vitamin B12, vitamin C, vitamin D, vitamin E, and carotenoids (provitamin A). In addition, excess alcohol consumption reduces energy intake (by decreasing appetite, causing nausea and vomiting), consumes energy and vitamins during its metabolisation by the liver, and also increases the elimination of metabolites by the kidney.
- Alcohol acts as a dissolvent and makes it easier for cells in the mouth and throat to absorb other cancer-causing chemicals, in particular those of the tobacco smoke.
- Alcohol can increase the levels of certain hormones in the body, including oestrogen. It is known that high levels of oestrogen can promote the development of breast cancer.
https://www.cancer.gov/about-cancer/causes-prevention/risk/alcohol/alcohol-fact-sheet
Several observational studies and meta-analyses, however, have also found a reduced incidence for certain cancers associated with light to moderate alcohol consumption. The mechanism by which this alcohol consumption may decrease the risks of some cancers is not completely understood and may be indirect and/or alcoholic beverage specific through anti-oxidant and anti-inflammatory effects.
2. Excessive consumption of alcoholic beverages and cancer risk
The association between the consumption of alcoholic beverages and the risk of certain cancers has been studied for several decades. These studies have found that the extent to which alcoholic beverages are a risk factor of a cancer depends significantly on the amount of alcohol consumed, type of alcoholic beverage and how it is consumed, that is the pattern of consumption, and probably also the dietary pattern in which alcohol is consumed.
Consumption levels and drinking patterns vary greatly between cultures and societies, however, and large amounts of an alcoholic beverage as well as regular heavy and binge drinking patterns generally impact on an individual’s health and welfare.
Excessive consumption of alcoholic beverages is a risk factor for certain types of cancer and the risk generally increases with increasing levels of consumption.
For example, there is evidence that regular heavy excessive consumption of alcoholic beverages and binge drinking patterns (Roerecke et al 2014) are associated with increased morbidity and mortality from certain cancers, and particularly cancers of the upper aero-digestive tract (such as the mouth, tongue, larynx, pharynx and oesophagus) (Pelucchi et al 2011).
This increased risk is especially seen among individuals who also smoke tobacco (Anantharaman et al 2011, Szymariska et al 2011). Alcohol and tobacco enhance each other’s effects (i.e. act synergistically) on the risk of cancers of the upper digestive and respiratory tract. Cancer of the liver can result from alcoholic liver cirrhosis, which is related to long-term heavy drinking (Parry et al 2011, White et al 2017; Jin et al 2013, Xi et al 2017) in conjunction with an unhealthy diet and/or hepatitis C and B virus infection.
Besides those cancers listed above, other malignancies shown to be associated with heavy drinking include colorectum cancer as well as female pre- and post-menopausal breast cancer (IARC Working Group 2018). These cancers are referred to as alcohol-attributable cancers, and there is sufficient or convincing evidence of the attributions (World Cancer Research Fund International 2018).
One of many meta-analyses relating the consumption of alcoholic beverages to all cancer mortality suggested, however, that for heavy drinkers (>50 g alcohol/d), the relative risk of dying from any cancer was increased by 32% (Jin et al 2013).
Binge drinkingBinge drinking (consuming rapidly four or more alcoholic drinks over a short period of time) has bee...
Binge drinkingBinge drinking (consuming rapidly four or more alcoholic drinks over a short period of time) has bee..., that is consuming rapidly four or more alcoholic drinks over a short period of time, has particularly been found to have a negative impact on health (Roerecke et al 2014, Chen et al 2011). This pattern of consumption results in a rapid and relatively sustained increase in the alcohol concentration circulating throughout the body and brain (Wechsler et al 1998). Such a high blood alcohol concentration (BAC) can impact on metabolic processes in response to alcohol drinking such as the formation of free radicals implicated in certain cancers (Brooks et al 2017). In these circumstances, the elimination of alcohol from the body via the enzymes ADH and ALDH may not be sufficiently effective (Seitz et al 2007) and a high BAC continues to circulate until it triggers the MEOS system to switch on, thereby increasing the capacity of the liver to eliminate the alcohol from the body. Thus, there is no doubt that binge drinkers have a high risk to develop cancer.
3. Moderate consumption of alcoholic beverages and cancer risk
While existing research is largely consistent as to the harms of heavy/excessive drinking in term of both cancer risk and overall mortality, there are disparate messages regarding the safety of light to moderate consumption of alcoholic beverages. Some argue that there is ‘no safe limit of alcohol’, mainly on the basis of an increased cancer risk (Wood et al 2018), and others emphasize the potential benefits for reducing cardiovascular mortality (Xi et al 2017).
Although excessive consumption has been linked to increased risk of several types of cancer, the overall effect of light to moderate consumption of alcoholic beverages on cancer incidence is less clear and findings are inconsistent (Zhou et al 2016). Whereas some studies have found a minimally increased or no increased risk of overall cancer (Xi et al 2017), others have found that even light and moderate drinking significantly contributes to an increased overall cancer risk (Bagnardi et al 2013, Bagnardi et al 2015, Cao et al 2015).
The overall cancer risk is difficult to evaluate since cancer consists of various diseases, each having specific characteristics.
Furthermore, some of the meta-analyses investigating the association between the consumption of alcoholic beverages and cancer risk have limitations that need to be considered when evaluating the cancer risk: they did not assess the different drinking patterns and types of alcoholic beverages in modifying the effect of the total amount of alcohol (Bagnardi et al 2015); in addition, underreporting of alcohol consumption may partly or largely explain the cancer risk with light drinking (Klatsky et al 2014)
A large prospective study found a J-shaped association between alcohol and mortality when examining the lifetime alcohol consumption in older adults, which remained after adjusting for the cancer risk. The lowest combined risk of death and cancer was observed for light alcohol intakes (between 1 and 5 drinks/week) in both men and women (Kunzmann et al 2018).
An assessment of risk for all cancer types by pooling the results of several epidemiological studies in a meta-analysis found a J-shaped curve between light to moderate drinking and overall cancer risk. This translated into a 9% lower risk of developing cancer for light drinkers (<12.5 g alcohol /d) compared to abstainers but an increased risk for excessive drinkers. No increased risk of dying from cancer for moderate drinkers (1-3 drinks/day) compared to abstainers (Jin et al 2013) was also reported.
A large meta-analysis reached similar conclusions that the consumption of alcoholic beverages (up to 1 drink/day) was not associated with the risk of most of the common cancers, except for the relatively small increase in the incidence of breast cancer in women and colorectal cancer in men (Choi et al 2018).
A comprehensive review of more than 7,000 peer-reviewed papers on the association of lifestyle factors and cancer undertaken by the World Cancer Research Fund in cooperation with the American Institute for Cancer Research (2007), reported that there are also alcohol threshold effects for colorectal cancer (CRC), the third most commonly diagnosed cancer worldwide (Bray et al 2018). Indeed, an increased risk for colorectal cancer is only apparent above a threshold of 30 g alcohol/day for both men and women (Cai et al 2014). In addition, a large meta-analysis of 16 studies observed a J-shaped dose-response relationship such that moderate alcohol consumption (1-2 alcoholic beverages/day) was associated with a reduced CRC risk compared to abstinence; consistent with other studies, risk of CRC increased with consumption of three or more drinks per day (McNabb et al 2020).
Another meta-analysis was carried out in an attempt to quantify the effect of moderate consumption of alcoholic beverages on overall cancer incidence in the Western world (Hendriks 2018). The authors wanted to estimate the overall cancer risk of the most common cancer types among men and women at light and moderate levels of alcohol consumption. The following was found:
- At light to moderate levels (up to 14.5 g alcohol/day), the overall effect of alcohol consumption on the risk of acquiring cancer was slightly lower in both men and women compared to non-drinkers (abstainers).
- At higher drinking categories (up to 60 g alcohol/day), the relative risk was slightly higher (5% for men and 10% for women) compared to non-drinking.
The overall cancer risk only increased substantially when drinking 60 g or more alcohol/day. - A gender difference in cancer risk was observed for a given amount of alcohol such that an increase in risk was observed at 22 g/day for women but at 46 g/day for men.
- Overall, the authors found that the light to moderate consumption of alcoholic beverages was not associated with a higher incidence of the 20 most common cancer types in the Western world in contrast to higher consumption.
Based on their results, Hendriks et al (2018) concluded that moderate drinking had no substantial impact on overall cancer risk. Moderate consumption of alcoholic beverages as such may therefore be considered as a less important lifestyle factor for affecting the overall cancer risk compared to other lifestyle factors, such as smoking and obesity. In contrast, heavy consumption, both regular and binge drinking of more than 60 g alcohol/day, is associated with an increased incidence for most types of cancer investigated in this present meta-analysis.
3.1 Breast cancer
Even though an increased overall cancer risk for women who drink moderately, was not shown by Hendriks et al (2018), it did indicate that women appear more sensitive to the pro-cancerous effects of alcohol.
Most observational, epidemiological studies have accordingly shown a small increase in the risk of breast cancer for women who consume any alcoholic beverages compared to non-drinkers. The degree of increase is usually small for light-to-moderate drinkers, between 5% and 10% increase in the relative risk for consumers of no more than one drink/day, but the risk may be higher for women consuming greater amounts (Bagnardi et al 2015, Fagherazzi et al 2015, Choi et al 2018).
Since breast cancer is the most common cancer among women in Western countries (Bray et al 2018), even a small increased breast cancer risk from light drinking women may be relevant.
3.2 Salient confounding factors
There are, however, several confounding factors in the breast-cancer – alcohol relationship as follows:
- pattern of drinking (regular versus binge) (Chen et al 2011, Giacosa et al, 2016, Liu et al 2015, Rehm et al 2019, Sanchez-Bayona et al 2020);
- type of alcoholic beverage (Bessaoud et al 2008, Shufeldt et al 2011);
- folate intake (Zeng et al 2019);
- hormone replacement therapy (HRT) hormones (Beral et al 2003, Sun et al 2017);
- no breast feeding;
- tobacco smoking (Viner et al 2019);
- genetic factors (such as BRC2 gene mutation) (Dennis et al 2011);
- obesity (Dennis et al 2011) and
- the dietary pattern (Schwingshackl et al 2017).
It has also been shown that the risk of breast cancer among obese women is higher than among non-obese women, but there are limited data on how obesity interacts with alcohol influencing the risk of breast cancer (Seiler et al 2018, Xiao et al 2019, van den Brandt et al 2000).
4. Cancer as a multifactorial disease and the importance of context
Since cancer is a multi-factorial disease, the cancer risk cannot be evaluated in isolation, and studies suggest that lifestyle factors are important risk factors for cancer (Kerr et al 2017). Accordingly, the consumption of alcoholic beverages cannot be accurately evaluated in insolation from the other risk factors (Teissedre 2020).
For example, when the risk from alcohol is assessed within the context of a balanced diet and a healthy lifestyle, the results seem to be very different (see below).
Indeed, the balance between genetic predisposition and environmental factors, including nutritional components and lifestyle behaviours, determines individual susceptibility to develop cancer (Khan 2010).
Only approximately 10 to 15% of alcohol dependent drinkers develop liver cirrhosis and, of those, only 10% develop liver cancer (Hall 1995). Similarly, not all heavy drinkers develop cancer, and some light-to-moderate drinkers develop cancer. This suggests that an individual’s genetic predisposition influences their risk of developing cancer and it has also been suggested for colorectal cancers; such that there is a stronger relationship between alcohol consumption and colorectal cancers among individuals with a family history of colorectal cancer (Cao et al. 2015).
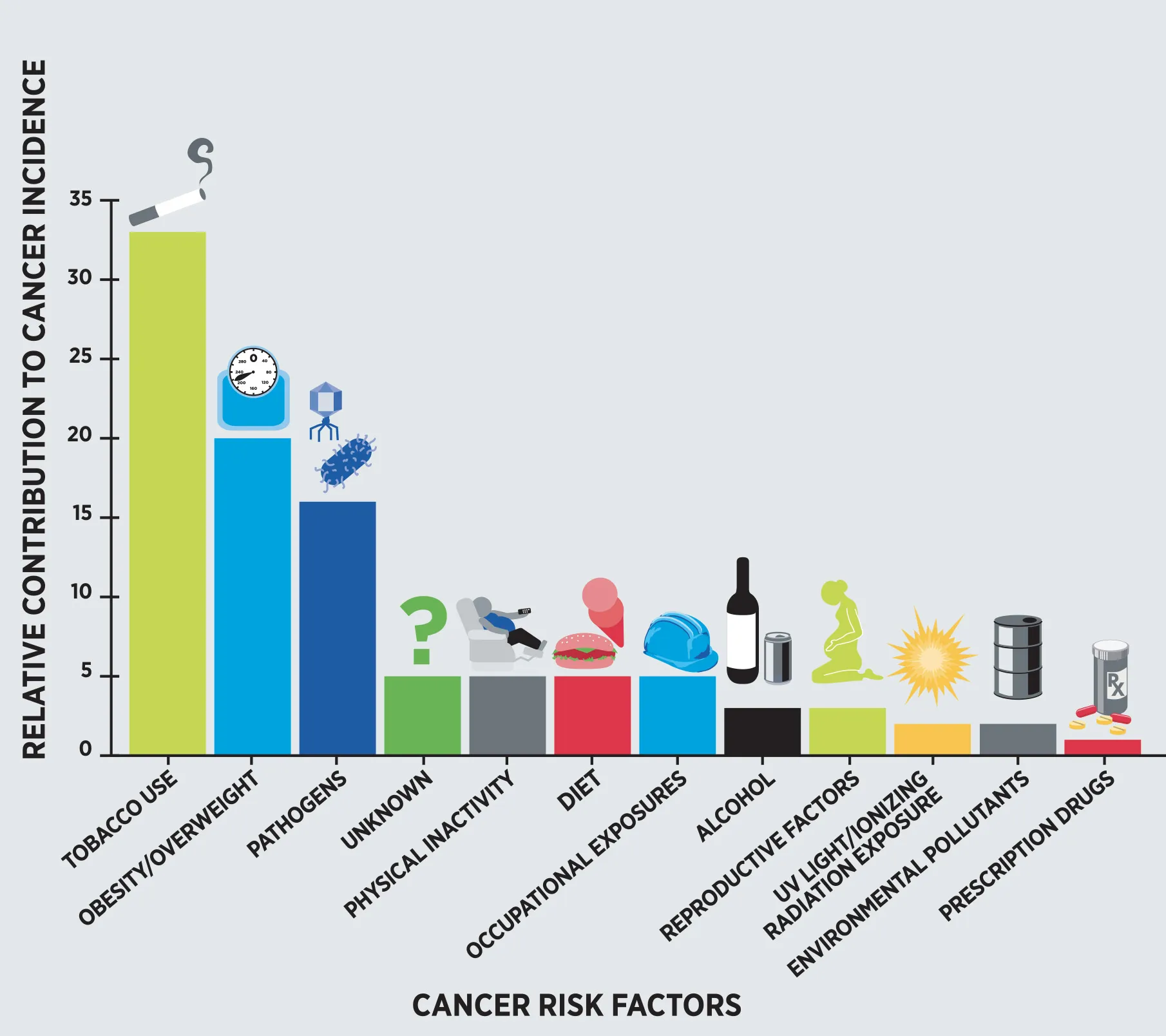
Smoking (30%), obesity (20%) and infections (15%) appear to account for a large proportion, while physical inactivity, an unhealthy diet and occupational hazards contribute 5% each, where the excessive consumption of alcoholic beverages contributes 3% to the overall cancer incidence (Fig. 1) (Arteaga et al 2014).
Thus, it is important to assess the cancer risk in context with its cultural, drinking and eating patterns and lifestyle influences, and also to remember that epidemiological studies cannot adequately control for all possible confounding factors such as social background, education, physical activity, eating and drinking pattern, and other unknown factors.
Should anyone be particularly careful?
Of all the alcohol-related cancers, breast cancer is the most common cancer in women. The risk of breast cancer increases with the number of drinks consumed daily in a dose-dependent manner where epidemiological studies show a linear increase in the relative risk of breast cancer with increasing amounts of alcohol. For a light to moderate amount of alcohol consumed, the magnitude of the effect is relatively small. Co factors play an important role in increasing risk, where an increased risk appears additive to, and especially observed in women with a genetic predisposition, with folate deficiencies, on hormone replacement therapy, overweight (Dennis et al 2010) and smoking. Within a healthy diet and lifestyle, risk of breast cancer can be minimised.
Women should be made aware of this risk, however, and if they decide to consume wine, then they should do so only moderately and always with the meals (Boban et al 2016) as part of a healthy diet and lifestyle.
Women should consult with their physicians/health care providers about their own risk.
5. Wine consumption as part of the Mediterranean Diet – risk in context
Long-term observational studies have also found differences between the alcoholic beverages. At low to moderate wine consumption, often no association with alcohol-related cancer types was observed. Especially when the risk was assessed in the context of other lifestyle factors, light to moderate wine consumption does not seem to be related to any increased cancer (and other disease) risk (Schwingshackl et al 2017, Li et al 2020).
The Mediterranean Diet (Med Diet), which includes moderate consumption of wine, is considered as one of the healthiest dietary pattern in the world by the WHO, noting that it is directly associated with a lower rate of mortality due to its effects on chronic disease prevention (WHO Europe 2018).
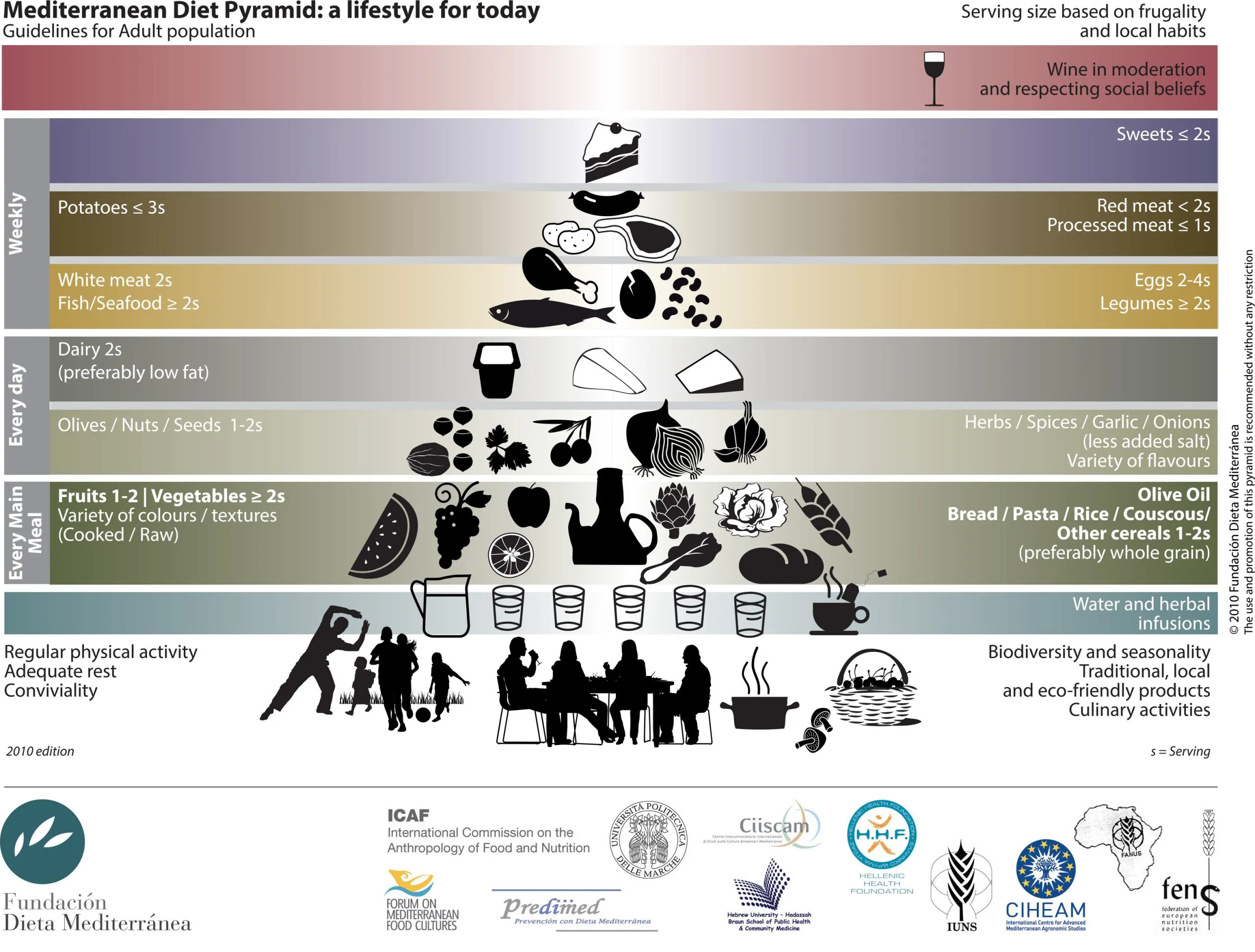
The Med Diet is characterized by:
- High intake of plant-based foods,
- Especially whole grain products,
- Fruits, vegetables, nuts, legumes,
- Regular intake fish and seafood,
- High intake of cereals, mainly whole grains,
- Fat is predominantly in form of extra virgin olive oil,
- Moderate intake of fish and poultry (white meat),
- Moderate consumption of alcohol, preferably wine with meals,
- Low amounts of dairy products and eggs as well as red meat and processed meat.
Taken together, this results in a dietary pattern with a low content of saturated fatty acids (7–8% of daily total energy consumption) and a total percentage of fat of 30–40% or greater per day (Schwingshackl et al 2019; Schwingshackl et al 2017, Sofi et al 2014, Willett et al 1995; Fidanza et al 2005).
5.1 Mediterranean drinking patternThe Mediterranean diet, which includes moderate consumption of wine, is considered ...
The Mediterranean drinking patternThe Mediterranean diet, which includes moderate consumption of wine, is considered ... is not only about the amount of alcoholic beverage consumed but also the type of alcoholic beverage predominantly consumed – wine – and how it is consumed.
Drinking patterns in terms of frequency and the amount of wine consumed as well as drinking with or without a meal are important influencing factors for the biological effects of this alcoholic beverage. Risky and harmful drinking patterns including the regular consumption of heavy amounts of wine, as well as consuming heavy and excessive amounts on a single occasion (binge drinking), should be discouraged. It is thus recommended that individuals drink wine as an accompaniment to food, and alternate it with a non-alcoholic beverage such as water (Boban et al 2016).
Spanish researchers examined the drinking patterns and concluded that the traditional Mediterranean drinking habits (such as moderate intake of alcoholic beverages, alcohol intake spread over the week, low spirit consumption, a preference for wine, wine consumed during meals, and avoidance of binge drinking) were also associated with a lower risk of all-cause mortality (Gea et al 2014).
5.2 Low to moderate wine consumption as part of a balanced diet such as the Med Diet
Intake of individual foods has been extensively studied in relation to cancer risk and for the chemical substance ethanol, a convincing evidence has been established, particularly for breast cancer (IARC 2012, WCRF 2018). However, individuals do not consume isolated foods or nutrients and examining dietary patterns in relation to cancer risk is consequently more meaningful
Thus, it should be emphasized that the effect of alcohol on the tumour development depends on the context. Diet has been identified as a modifiable lifestyle component that influences the cancer development. The Med Diet is considered one of the healthiest diet because of its abundance of plant-based foods and the lack of processed foods (Willett et al 1995). Numerous epidemio¬logical studies (Pellucchi et al 2009, Eleftheriou et al 2018, Soltani et al 2019 (Schwingshackl, Morze et al. 2020) have focused on the health effects of the Med Diet, where studies that have examined the role of wine in the Mediterranean diet have identified a decreased risk of multiple health outcomes.
5.3 Med diet and all-cause mortality
More adherence to a Mediterranean dietary pattern resulted in: a reduced risk of all-cause mortality, cardiovascular diseases, coronary heart disease, stroke, overall cancer, diabetes and neuro-degenerative incidence (Dinu et al 2018, Soltani et al 2019).
An updated meta-analysis quantified the association of adherence to the Med Diet and all of its components with all-cause mortality (Eleftheriou et al 2018). When looking at the Med Diet components, a statistically significant inverse association was highlighted for a moderate consumption of alcoholic beverages compared to abstinence or excessive consumption.
5.4 Med Diet and cancer risk
The extent to which different drinking and dietary patterns, lifestyle habits and/or beverage specific ingredients are responsible for the observed reduced risk of certain cancers continues to be discussed, and may provide an explanation as to why no increased breast cancer risk has generally been observed within the context of a Med Diet (Trichopoulou et al 2010, Cade et al 2011, Couto et al 2011, Toledo et al 2015, Morze, Danielewicz et al. 2020, Molina-Montes, Ubago-Guisado et al. 2021).
When examining moderate wine consumption in the context of the Mediterranean diet and typically with the meals, no increased cancer risk, even for breast cancer (Schwingshackl et al 2017, Toledo et al 2015) was observed. Furthermore, a better adherence to the Med Diet was also associated with a lower risk total mortality, that is dying from any cause (Soltani et al 2019).
The above results were confirmed by large meta-analyses, where a greater adherence to the Med Diet was associated with a lower cancer risk (Schwingshackl et al 2017, Galbete et al 2018). When focusing specifically on prospective trials, this meta-analysis highlighted decreases in the risk of suffering colorectal and breast malignancies and in cancer mortality among subjects with high Med Diet adherence. In line with these findings, a randomized controlled trial has studied the effect of this dietary pattern on cancer incidence. Adherence to the traditional Med Diet in the context of the PREDIMEDThe PREDIMED study is one of the few randomized controlled trials about the Mediterranean Diet. More... Study demonstrated a decrease in the development of all sub-types of breast cancer and a decrease in its recurrence (Toledo et al 2015). Such results need to be confirmed in further long-term trials.
Regarding the alcohol, as stated by Schwingshackl et al. (2017), the attribution of anti-cancer effects to its consumption seems controversial, considering that it is categorized by the IARC as a Group 1 carcinogen for humans (IARC 2012) and by the World Cancer Research Fund as a convincing carcinogen for mouth, pharynx, larynx, esophagus, stomach, liver, colorectal, and breast malignancies (WRCF 2018). Low-to-moderate wine consumption contributes, however, to a higher Med Diet adherence (linked to the previously described benefits) and no dose-response effect of the toxicity of alcohol or wine consumption can be inferred from their conclusions.
5.5 Wine – a protective component of the Med Diet
The inclusion of alcohol in the Med Diet usually means moderate wine consumption as part of a meal (Gea et al 2014). When analysing the components of the Med Diet that contributed most to such a decreased cancer risk, researchers have specifically identified the moderate, but not excessive consumption of alcoholic beverages and predominantly wine, fruits, vegetables and whole grains as protective components (Schwingshackl et al 2017, Eleftheriou et al 2018).
There is sufficient clinical evidence to point out that moderate wine drinkers have a lower risk for cancer compared to drinkers of other alcoholic beverages. So far, the anti-cancer effects of wine-specific polyphenols have only been observed in animal and laboratory studies. In some epidemiological studies, however, the risk of cancer has been shown to be lower in wine drinkers than in those who consumed other alcoholic beverages (Xu et al 2019, Groenbaek M et al 2000).
5.6 Possible mechanisms
Wine provides large amounts of several bioactive compounds such as polyphenols that may be potentially responsible for some of the wine’s anti-cancer effects (Fernandes et al 2017) and the possible counter effects of the entire dietary composition of a Med Diet against the toxicity of alcohol on cancer has not been explored (Hernaez A et al 2019). Thus, the observed positive health effects of light to moderate wine consumption may be – at least in part – linked to the protective effects of specific bioactive ingredients in the wine (polyphenols) as well as in the foods consumed with higher abundance in the Mediterra¬nean diet (Eleftheriou et al 2018 (Schwingshackl, Morze et al. 2020)).
PolyphenolsPolyphenols are mainly phytochemicals found abundantly in natural plant food sources. The most impor...
Wine contains phenolic compounds (polyphenols) which give wine its characteristic colour and flavour and are produced by plants in response to fungal infection, and various chemical and physical stressors, especially during ripening. They are extracted from the seeds and skins of grapes during fermentation of winemaking, when the juice is in contact with the grape skins and seeds. The amount of polyphenols in red wine is generally greater than in white wine because the red juice has longer contact with the grape skins during fermentation enabling more phenolic substances to be extracted into the red juice.
There is evidence that certain wine-derived phenolic compounds, such as resveratrol, and flavonoids such as anthocyanins, catechins and flavanols can provide health benefits. Researchers have shown that wine-derived phenolic compounds act as antioxidants and stimulate antioxidant defense systems (Forman et al 2014). Thereby, these antioxidants are believed to reduce the damage caused by the body’s free radicals (toxic waste products) which contribute to causing degenerative diseases in the body such as cancer, Alzheimer’s disease, Parkinson’s disease, and general ageing.
Many polyphenols are metabolised by gut bacteria. Recently, it has been shown that rather than the polyphenols themselves, their metabolites might be the key compounds in cardiovascular and cancer protection (Yang et al 2020).
Resveratrol
Resveratrol is a naturally occurring phenolic compound in red wine that provides a number of anti-aging health benefits. As a natural food ingredient, numerous animal and laboratory studies have demonstrated that resveratrol shows a high antioxidant activity. Resveratrol also exhibits antitumor activity and is considered a potential candidate for prevention and treatment of several types of cancer. Other observed bioactivity includes anti-inflammatory, anti-carcinogenic, cardio-protective, vasorelaxant and neuroprotective effects. Although resveratrol can inhibit the growth of cancer cells in experimental and animal models, it is not known whether resveratrol can prevent and/or help treat cancer in humans (Carter et al 2014, Ramirez-Garza et al 2018, Salehi et al 2018).
6. Moderate wine consumption and cancer risk in context (“umbrella”) of a healthy lifestyle
Several studies confirm that adopting a healthy lifestyle and a balanced diet, including a moderate consumption of wine/alcoholic beverages, has a number of positive and protective health effects.
6.1 More years without chronic diseases
A large study from Harvard University examined comprehensively how multiple lifestyle factors relate to life expectancy without major diseases and confirmed these recommendations: following a healthy lifestyle at mid-life is associated with a longer life expectancy and a lower risk of major diseases such as cancer, cardiovascular and diabetes. The study highlights five specific lifestyle factors, one of them is the moderate consumption of alcoholic beverages (Li et al 2020):
Five Lifestyle Factors:
- Never smoking
- Normal body weight (BMI 18.5 – 24.9)
- Moderate to vigorous physical activity
- Moderate consumption of alcoholic beverages (women 5-15g/day, men 15-30g/day)
- Balanced diet
The researchers found that women (at age 50) who ate a healthy diet, exercised 30 minutes each day, had a normal body weight and consumed alcoholic beverages in moderation lived to an average of 84.4 years old without developing diabetes, cardiovascular disease and cancer. Those women who did not practice these healthy habits were more likely to develop those diseases in their 70s. Middle-aged men practising these habits lived to an average of 81.1 years old without chronic diseases compared to 73.5 years old for men who did not.
Thus, in the context of a healthy lifestyle, moderate wine/alcohol consumption is one lifestyle factor that contributes to a longer life expectancy free of major diseases (Li et al 2020).
6.2 Longer life expectancy
The same Harvard researchers (Li et al 2018) (Fig. 3) had already shown earlier that those five lifestyle factors could increase the life expectancy. They were surprised how immense the benefits of all these five lifestyle factors would be:
- 50 year old women who would practice ALL these healthy lifestyle factors could enjoy 14 additional years (93 instead of 79 years) and
- 50 year old men would benefit with 12 additional years (87 instead of 75 years).
- The reference group consisted of individuals with none of these lifestyle factors.
- Compared to this group, the mortality risk was 74% lower when all 5 factors would be followed, the cancer risk was 65% lower and the CVD risk was 82% lower.
One of the five lifestyle factors – a moderate amount of alcoholic beverages – was defined for women 5-15 g of alcohol/day or the equivalent of 50 to 150 ml of wine and for men, 5-30 g of alcohol/day or the equivalent of 50 to 300 ml of wine.

A recent large European study reported similar results (Nyberg et al 2020), where the higher the number of healthy lifestyle habits, the longer the lifespan without major chronic diseases (type 2 diabetes, coronary heart disease, stroke, cancer, asthma, chronic obstructive pulmonary disease, heart failure, dementia*). The longest life span free of disease was observed among those participants with a normal weight (BMI < 25) and two of the following lifestyle factors: never smoking, physical activity and moderate consumption of alcoholic beverages (1-14 drinks per week for women and 1-21 drinks per week for men).
Even the World Cancer Research Fund recently stated five lifestyle factors that contribute to a lower cancer risk (WCRF 2018), among them a healthy diet, including moderate wine/alcoholic beverage consumption.
(*)These specific diseases were selected because they are the most common major non-communicable diseases in developed countries and targets prioritised for global disease prevention by WHO (Gakidou et al 2018)
References
- Anantharaman D et al, 2011. Population attributable risk of tobacco and alcohol for upper aerodigestive tract cancer. Oral Oncol. 47: 725–731.
- Arteaga J et al, 2014, AACR Cancer Progress Report 2014, doi: 10.1158/1078-0432.CCR-14-2123
- Bagnardi V et al, 2013, Light alcohol drinking and cancer: A meta-analysis. Annals of Oncology, 24(2), 301-308
- Bagnardi V, et al., Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. British Journal of Cancer, 2015. 112(3): p. 580-593
- Bessaoud F et al, 2008, Patterns of alcohol (especially wine) consumption and breast cancer risk: a case-control study among a population in Southern France, Ann Epidemiol. 2008 Jun;18(6):467-75. doi: 10.1016/j.annepidem.2008.02.001
- Boban M et al, 2016, Drinking pattern of wine and effects on human health: why should we drink moderately and with meals? Food Funct 7: 2937
- Bray F et al 2018, Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries, CA CANCER J CLIN 2018;68:394–424, doi: 10.3322/caac.21492
- Brooks PJ et al 2013, Moderate alcohol consumption and breast cancer in women: from epidemiology to mechanisms and interventions. Alcohol Clin Exp Res. ;37(1):23–30
- Cade JE et al, 2011, Does the Mediterranean dietary pattern or the healthy diet index influence the risk of breast cancer in a large British cohort of women. Eur. J. Clin. Nutr. 2011, 65, 920–928.
- Cai S et al 2014, Alcohol drinking and the risk of colorectal cancer death: a meta-analysis, Eur J Cancer Prev. 2014 Nov;23(6):532-9. doi: 10.1097/CEJ.0000000000000076
- Cao Y et al, 2015. Light to moderate intake of alcohol, drinking patterns, and risk of cancer: results from two prospective US cohort studies. BMJ 351:h4238; doi: https://doi.org/10.1136/bmj.h4238.
- Carter LG et al 2014, Resveratrol and cancer: focus on in vivo evidence, Endocrine-Related Cancer 21, R209–R225
- Cederbaum A, 2012, Alcohol metabolism, Clin Liver Dis. 2012 Nov;16(4):667-85. doi: 10.1016/j.cld.2012.08.002
- Chen WY et al, 2011, Moderate alcohol consumption during adult life, drinking patterns, and breast cancer risk, JAMA;306(17):1884-90, doi: 10.1001/jama.2011.1590
- Choi YJ et al, 2017, Light Alcohol Drinking and Risk of Cancer: A Meta-analysisA meta-analysis is a method of summarizing the results of the same research purpose and comprehensiv... of Cohort Studies. Cancer Research and Treatment, 50(2):474-487. doi: 10.4143/crt.2017.094
- Couto E et al, 2011, Mediterranean dietary pattern and cancer risk in the EPIC cohort, Br J Cancer. 2011 Apr 26; 104(9): 1493–1499. doi: 10.1038/bjc.2011.106
- Dennis J, 2011, Breast cancer risk in relation to alcohol consumption and BRCA gene mutations–a case-only study of gene-environment interaction. Breast J.;17(5): 477-484
- Dinu M et al, 2018, Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials, Eur J Clin Nutr. 2018 Jan;72(1):30-43. doi: 10.1038/ejcn.2017.58
- Eleftheriou D et al, 2018, Mediterranean diet and its components in relation to all-cause mortality: meta-analysis, Br J Nutr. 120, 1081
- Fagherazzi G et al, 2015, Alcohol consumption and breast cancer risk subtypes in the E3N-EPIC cohort, Eur J Cancer Prev, Vol 24,3:209-214, doi: 10.1097/CEJ.0000000000000031
- Fernandes, I et al, 2017, Wine FlavonoidsFlavonoids represent a structurally diverse group of polyphenolic bioactive compounds found in many ... in Health and Disease Prevention. Molecules 2017, 22, 292
- Fidanza F et al, 2005, The Nicotera diet: The reference Italian Mediterranean diet. World Rev. Nutr. Diet. 95, 115–121
- Ford ES et al, 2011, Low-risk lifestyle behaviors and all-cause mortality: findings from the National Health and Nutrition Examination Survey III Mortality Study. Am J Pub Health. 101:1922–1929
- Forman HJ et al, 2014, Para-hormesis: An innovative mechanism for the health protection brought by antioxidants in wine Nutrition and aging 2(2014) 117-124
- Galbete C et al 2018, Evaluating Mediterranean diet and risk of chronic disease in cohort studies: an umbrella review of meta-analyses, Eur J Epidemiol. 2018 Oct;33(10):909-931. doi: 10.1007/s10654-018-0427-3
- Gakidou E et al 2018, Alcohol use and burden for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016
- Gea A et al, 2014, Mediterranean alcohol-drinking pattern and mortality in the SUN (Seguimiento Universidad de Navarra) Project: a prospective cohort study, Br. J. Nutr, 11 (10): 1871
- Giacosa A et al, 2016, Mediterranean Way of Drinking and Longevity, Crit Rev Food Sci Nutr. 2016;56(4):635-40. doi: 10.1080/10408398.2012.747484
- Gressner AM et al, 2019, Mikrosomales Ethanol-oxidierendes System. In: Gressner A.M., Arndt T. (eds) Lexikon der Medizinischen Laboratoriumsdiagnostik. Springer Reference Medizin. Springer, Berlin, Heidelberg
- Gronbaek M et al, 2000, Type of alcohol consumed and mortality from all causes, coronary heart disease, and cancer, Ann. Intern. Med 133 (6): 411
- Hall P, 1995, Pathological spectrum of alcoholic liver disease. In: Hall, P., ed. Alcoholic Liver Disease: Pathobiology and Pathogenesis, 2nd ed. London: Edward Arnold; 41–68
- Hendriks H et al 2018, The Contribution of Alcohol Consumption to Overall Cancer Incidence in the Western World: A Meta-Analysis, J Nutr Health Sci 5(3): 308. doi: 10.15744/2393-9060.5.308
- International Agency for Research on Cancer (IARC), Volume 100E: Personal habits and indoor combustions, in IARC Monographs on the evaluation of carcinogenic risks to humans. 2012.
- Jin M et al , 2013, Alcohol drinking and all cancer mortality: a meta-analysis. Ann;24(3):807-16.
- Khan N et al, 2010, Lifestyle as a risk factor for cancer: evidence from human studies, Cancer Lett. 2010 July 28; 293(2): 133–143. doi:10.1016/j.canlet.2009.12.013.
- Kerr J et al, 2017, Physical activity, sedentary behaviour, diet, and cancer: an update and emerging new evidence, Lancet Oncol. 2017 Aug;18(8):e457-e471. doi: 10.1016/S1470-2045(17)30411-4
- Klatsky et al, 2014, Moderate alcohol intake and cancer: the role of underreporting, Cancer Causes Control (6):693-9, doi: 10.1007/s10552-014-0372-8
- Kunzmann AT et al, 2018, The association of lifetime alcohol use with mortality and cancer risk in older adults: a cohort study, PLOS Medicine, https://doi.org/10.1371/journal.pmed.1002585
- Li Y et al, 2018, Impact of healthy lifestyle factors on life expectancies in the US population, Circulation;137:00–00. DOI: 10.1161/CIRCULATIONAHA.117.032047
- Li Y et al , 2020, Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: prospective cohort study, BMJ;368:l6669 | doi: 10.1136/bmj.l6669
- Liu Y et al 2015, Links between alcohol consumption and breast cancer: a look at the evidence, Womens Health 11(1), 65-77, doi:10.2217/WHE.14.62
- McNabb S et al, 2020, Meta-analysisA meta-analysis is a method of summarizing the results of the same research purpose and comprehensiv... of 16 studies of the association of alcohol with colorectal cancer, Int. J. Cancer: 00, 00–00
- Mørch LS et al, 2007, Alcohol drinking, consumption patterns and breast cancer among Danish nurses: a cohort study. Eur. J. Public Health. 17(6): 624-629
- Molina-Montes, E., E. Ubago-Guisado, D. Petrova, P. Amiano, M. D. Chirlaque, A. Agudo and M. J. Sanchez (2021). “The Role of Diet, Alcohol, BMI, and Physical Activity in Cancer Mortality: Summary Findings of the EPIC Study.” Nutrients 13(12).
- Morze, J., A. Danielewicz, K. Przybylowicz, H. Zeng, G. Hoffmann and L. Schwingshackl (2020). “An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer.” Eur J Nutr.
- Newman TM et al, 2019, From the Table to the Tumor: The Role of Mediterranean and Western Dietary Patterns in Shifting Microbial-Mediated Signaling to Impact Breast Cancer Risk, Nutrients, 11, 2565; doi:10.3390/nu11112565
- Nyberg S et al, 2020, Association of Healthy Lifestyle With Years Lived Without Major Chronic Diseases, JAMA Intern Med. doi:10.1001/jamainternmed.2020.0618
- Parry CD et al, 2011, Alcohol consumption and non-communicable diseases: epidemiology and policy implications, Addiction 106: 1718-24
- Peila, R., R. S. Arthur, A. J. Dannenberg and T. E. Rohan (2022). “Association of a Healthy Lifestyle Index with Risk of Breast Cancer among Women with Normal Body Mass Index in the UK Biobank.” Cancer Epidemiology, Biomarkers & Prevention: OF1-OF7.
- Pelucchi C et al, 2009, Selected aspects of Mediterranean diet and cancer risk, Nutr Cancer. 2009;61(6):756-66. doi: 10.1080/01635580903285007
- Pelucchi et al, 2011, Alcohol consumption and cancer risk, Nutrition and Cancer, 63 (7):983-990, doi:10.1080/01635581.2011.596642
- Perreault K et al, 2017, Does physical activity moderate the association between alcohol drinking and all-cause, cancer and cardiovascular diseases mortality? A pooled analysis of eight British population cohorts, Br J Sports Med;51:651-657
- Ramírez-Garza S et al, 2018, Health Effects of Resveratrol: Results from Human Intervention Trials, Nutrients 2018, 10, 1892; doi:10.3390/nu10121892
- RehmJ et al, 2019, Does alcohol use affect cancer risk?, Curr Nutr Rep, https://doi.org/10.1007/s13668-019-0267-0
- Roerecke et al, 2014, Alcohol consumption, drinking patterns, and ischemic heart disease: a narrative review of meta-analyses and a systematic review and meta-analysis of the impact of heavy drinking occasions on risk for moderate drinkers, BMC Med. 2014; 12: 182. doi: 10.1186/s12916-014-0182-6
- Salehi B et al, 2018, Resveratrol: A Double-Edged Sword in Health Benefits, Biomedicines 2018, 6, 91; doi:10.3390/biomedicines6030091
- Sanchez-Bayona R et al, 2020, Binge Drinking and Risk of Breast Cancer: Results from the SUN (‘Seguimiento Universidad de Navarra’) Project, Nutrients 12(3). pii: E731. doi: 10.3390/nu12030731
- Schwingshackl, L., J. Morze and G. Hoffmann (2020). “Mediterranean diet and health status: Active ingredients and pharmacological mechanisms.” Br J Pharmacol 177(6): 1241-1257.
- Schwingshackl L et al, 2019, Mediterranean diet and health status: Active ingredients and pharmacological mechanisms, Br J Pharmacol. 2020;177:1241–1257
- Schwingshackl L et al, 2015, Adherence to Mediterranean diet and risk of cancer: a systematic review and meta-analysis of observational studies. Int J Cancer. 2014 Oct 15;135(8):1884-97. doi: 10.1002/ijc.28824
- Schwingshack, L et al, 2015, Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. , 4, 1933–1947.
- Schwingshackl L et al, 2017, Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis, Nutrients. 2017 Sep 26;9(10). pii: E1063. doi: 10.3390/nu9101063
- Seiler A et al 2018, Obesity, Dietary Factors, Nutrition, and Breast Cancer Risk, Curr Breast Cancer Rep. 2018 Mar; 10(1): 14–27, doi: 10.1007/s12609-018-0264-0
- Seitz HK et al 2007, Alcohol metabolism and cancer risk, Alcohol Res Health. 2007;30(1):38–41.
- Sofi F et al, 2014, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. , 17, 2769–2782
- Soltani S et al, 2019, Adherence to the Mediterranean Diet in Relation to All-Cause Mortality: A Systematic Review and Dose-ResponseMeta-Analysis of Prospective Cohort Studies, Adv Nutr 2019;10:1029–1039; doi: https://doi.org/10.1093/advances/nmz041
- Stockley C et al, 2010, The biology of intoxication. In: Fox, A., MacAvoy, M. (eds.) Expressions of Drunkenness (Four Hundred Rabbits). Routledge, New York. pp. 13–52
- Stroehle A et al, 2012, Alcohol intake–a two-edged sword. Part 1: metabolism and pathogenic effects of alcohol, Med Monatsschr Pharm. 2012 Aug;35(8):281-92
- Szymańska K et al, 2011, Alcohol and tobacco, and the risk of cancers of the upper aerodigestive tract in Latin America: a case–control study. Cancer Causes Control. 22: 1037–1046.
- eissedre, P. R.-P., Z.; Ruf, J.; Stockley, C.; Antoce, A.O.; Romano, R.; Fradera, U.; Kosti, R.I. (2020). “Effects of alcohol consumption in general, and wine in particular, on the risk of cancer development: a review.” OENO one 54(4).
- Toledo E et al, 2015, Mediterranean Diet and Invasive Breast Cancer Risk Among Women at High Cardiovascular Risk in the PREDIMEDThe PREDIMED study is one of the few randomized controlled trials about the Mediterranean Diet. More... Trial: A Randomized Clinical Trial. JAMA Intern Med , 175, 1752–1760
- Trichopoulou A et al, 2009, Anatomy of health effects of Mediterranean diet: Greek EPIC prospective cohort study, : BMJ;338:b2337, doi:10.1136/bmj.b2337
- Trichopoulou A et al, 2010, Conformity to traditional Mediterranean diet and breast cancer risk in the greek EPIC (European Prospective Investigation into Cancer and Nutrition) cohort. Nutr. Clin. Pract., 25, 682–684.
- Turati F et al, 2020, Adherence to the World Cancer Research Fund/American Institute for Cancer Research Recommendations and the Risk of Breast Cancer, Nutrients 2020, 12, 607
- Van den Brandt PA et al, 2000, Pooled analysis of prospective cohort studies on height, weight, and breast cancer risk. Am J Epidemiol 152:514‐527
- Van den Brandt P et al, 2017, Mediterranean diet adherence and risk of postmenopausal breast cancer: results of a cohort study and meta-analysis, Int J Cancer, 140, 2220–2231
- Viner B et al, 2019, The individual and combined effects of alcohol consumption and cigarette smoking on site- specific cancer risk in a prospective cohort of 26,607 adults: Results from Alberta’s Tomorrow Project, Cancer Causes & Control, https://doi.org/10.1007/s10552-019-01226-7
- Wechsler H et al, Binge drinkingBinge drinking (consuming rapidly four or more alcoholic drinks over a short period of time) has bee...: the five/four measure. J Stud Alcohol. 1998;59(1):122–124
- World Health Organisation (WHO) and International Agency for Research on Cancer (IARC), Alcohol drinking. IARC Working Group, Lyon, 13-20 October 1987. IARC Monographs on the Evaluation of Carcinogenic Risks to Human, 1988. 44: 1-378.
- WHO, ‘Best buys’ and other recommended interventions for the prevention and control of non-communicable diseases. https://www.who.int/iris/handle/10665/259232 ,2017.
- WHO Europe 2018, Health Evidence Network synthesis report 58.
- World Cancer Research Fund/American Institute for Cancer Research, Continuous update project expert report 2018. Recommendations and public health and policy implications. https://www.wcrf.org/sites/default/files/Cancer-Prevention-Recommendations-2018.pdf , 2018
- WCRF/AICR, 2007, Expert Report, Food, Nutrition, Physical Activity and the Prevention of Cancer: a Global Perspective
- World Cancer Research Fund (WCRF) and American Institute for Cancer Research (AICR), Continuous Update Project Expert Report 2018. Alcoholic drinks and the risk of cancer. 2018.
- WHO . Cancer Prevention. Available online: https://www.who.int/cancer/prevention/en
- Willett WC et al, 1995, Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr., 61, 1402S–1406S
- Wood AM, et al. 2018 : Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies in Lancet 2018; 391: 1513-23
- Xi et al, 2017, Relationship of Alcohol Consumption to All-Cause, Cardiovascular, and Cancer-Related Mortality in U.S. Adults, J Am Coll Cardiol 2017;70:913–22
- Xiao Y et al, 2019, Associations between dietary patterns and the risk of breast cancer: a systematic review and meta-analysis of observational studies, Breast Cancer Research (2019) 21:16 https://doi.org/10.1186/s13058-019-1096-1
- Xu W et al, 2019, Wine consumption and colorectal cancer risk: a meta-analysis of observational studies, Eur J Cancer Prev. 2019 May;28(3):151-158. doi: 10.1097/CEJ.0000000000000444
- Yang Q et al, 2020, Role of Dietary Nutrients in the Modulation of Gut Microbiota: A Narrative Review, Nutrients 2020, 12, 381; doi:10.3390/nu12020381
- Zhang Y et al, 2020, Combined lifestyle factors and risk of incident type 2 diabetes and prognosis among individuals with type 2 diabetes: a systematic review and meta-analysis of prospective cohort studies, Diabetologia (2020) 63:21–33, https://doi.org/10.1007/s00125-019-04985-9
- Zeng J et al, 2019, Folate intake and the risk of breast cancer: an up-to-date meta-analysis of prospective studies, Eur J Clin Nutr, https://doi.org/10.1038/s41430-019-0394-0
